
Listen and Download Dr. Zourdos’ Personalized Audio File Below
Listen and Download The Text-To-Speech File Below
by Michael C. Zourdos
The media has been hyping the benefits of creatine for brain health. Is the hype real? If so, does this extend to clinical conditions such as Alzheimer’s disease? This article discusses the first human trial of creatine in patients with Alzheimer’s disease.
Key Points
- 20 women (n = 7) and men (n = 13) taking medication for Alzheimer’s disease (AD) consumed 20 g/d of creatine monohydrate for eight weeks to complete the first-ever human trial examining creatine supplementation in AD patients.
- The participants did not experience any severe adverse events, demonstrating the safety and feasibility of creatine. Furthermore, brain creatine content increased (~11%), and various measures of cognitive function improved.
- Without a control group for comparison causality cannot be confirmed from this single-arm study. However, it provides evidence of the feasibility and safety of creatine in AD patients and serves as hypothesis-generating research for future randomized controlled trials.
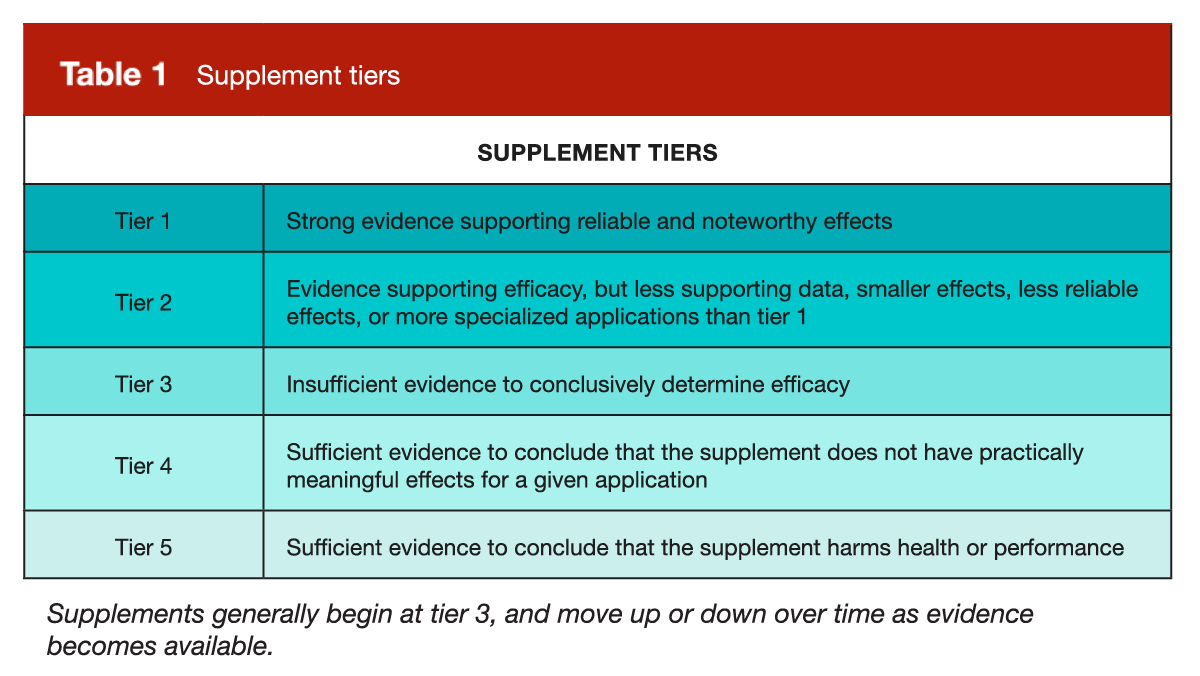
In Dr. Trexler’s unassailable supplement tiers, creatine stands alone as the only tier 1 supplement. This classification is with good reason as creatine’s efficacy (2) and safety (3) are well documented and remain unrivaled. Creatine earned this classification because of its impact on muscular performance and size via improved ATP resynthesis in muscle, but over the past decade there has been significant conversation about creatine boosting brain health and potentially having neuroprotective properties.
{kind=link}
Evidence is mixed regarding the role of creatine in cognition in young healthy individuals without cognitive impairment (4, 5 – MASS Review), which should not be surprising. However, the theory of creatine-boosting brain function has merit. As we age and experience mitochondrial dysfunction, ATP production tends to decrease, which is associated with cognitive impairment (6, 7). In the year 2000 (8), it was reported that brain creatine levels were related to memory, and more recently, a systematic review by Prokopodis et al (9) found that older individuals (66 – 76 years old) experienced significantly greater improvements in memory from creatine supplementation than younger individuals (11 – 31 years old). Due to the benefits of creatine in older adults and those with cognitive impairment, researchers wondered whether creatine supplementation could be useful for cognitive diseases such as Alzheimer’s disease (AD).
Individuals with AD have amyloid-beta peptides that disrupt mitochondrial production and subsequently impair ATP production (10). Thus, it’s logical that creatine supplementation can boost ATP production and cognition in patients with AD. In mice, studies have shown that creatine supplementation significantly increases ATP levels, with a concomitant decrease in amyloid-beta peptides. The potential benefits of creatine in patients with AD are potentially significant and range from improving cognition, increasing quality of life, and increasing lifespan. The reviewed study from Smith et al (1) is the first study to examine creatine supplementation in AD patients.
Purpose and Hypotheses
Purpose
The reviewed study was an observational trial investigating the feasibility of creatine supplementation and changes in cognitive performance and brain creatine levels over eight weeks in AD patients currently taking AD medication.
Hypotheses
The researchers hypothesized that creatine supplementation would be feasible, and that patients would experience increased brain creatine and cognition after the 8-week study.
Subjects and Methods
Subjects
20 individuals with AD (women, n = 7; men, n = 13; age = 73.1 ± 6.3 years) aged 60 – 90 years participated in this study. Subjects were only included if they scored ≥ 17 on the Mini-Mental State Examination (MMSE). The MMSE is an 11-item questionnaire with 30 points aimed at assessing cognition (11). A score below 17 indicates “severe” cognitive impairment, meaning all participants had (at worst) mild cognitive impairment. Subjects were also required to have been taking an AD medication for at least 30 days before the study. Further details of the subjects are presented in Table 1.

This study was a single-arm observational trial, which means all subjects received the same treatment and measurements were assessed over time. Specifically, all subjects were asked to ingest 20 g/d of creatine monohydrate split into two 10 g/d doses. The subjects ingested creatine at home and stirred it into a drink of choice. They were also provided with education related to creatine consumption by a dietitian and weekly phone call reminders to assist with complying with the protocol. Serum and brain creatine levels were assessed before and after the study. Cognitive function was assessed using various questionnaires from the NIH Cognitive Toolbox (12), which is a battery of assessments across various cognitive domains. Additionally, apolipoprotein E (APOE) genotyping and the biomarker p-tau217, which are both indicative of AD, were assessed at baseline to determine the presence of AD.

Findings
The main findings are as follows:
- Most participants were genetically predisposed to AD and had high levels of p-tau217.
- There were not any serious adverse events, only minor issues “which included cramping/muscle pain, diarrhea, constipation, nausea, facial flushing, and sleep disturbance.”
- Both serum and brain creatine levels increased over the 8 weeks.
- Individuals’ cognition improved in most assessments.
APOE Genotype and Tau Protein
Thirteen of the 20 subjects carried the ε4 allele, which is a genetic risk factor for AD. For p-tau217, data were collected from 19 of the 20 subjects. Of those 19 subjects, 18 had p-tau217 levels above 0.4 pg/mL, which suggests high amyloid-beta and the presence of AD.
Creatine Levels
Both serum and total brain creatine levels increased significantly over the course of the study (Table 3). Furthermore, changes in serum and brain creatine levels were significantly correlated (r = 0.49, p = 0.004).

Cognition
Most cognitive measures significantly improved from pre- to post-study, including total cognition, fluid cognition, list-sorting working memory, oral reading cognition, and the flanker test. I averaged all those raw scores and reported them in Figure 1. The pre- to post-study changes for all NIH Toolbox cognitive assessments and the associated percentage changes are shown in Table 4.


Interpretation
What Can We Determine from a Single-Arm Trial?
The reviewed study (1) was a single-arm trial, even being pre-registered specifically as a “single-arm pilot trial” (13). Thus, it is crucial to note what we can and cannot determine from this research design. In brief, single arm trials do not have a control group (i.e., a group of patients with AD who did not receive creatine supplementation). The lack of a control group means that we don’t know what would have happened without supplementation, so we cannot definitively determine that creatine supplementation caused the increased creatine levels or cognition. A control group essentially isolates the effect of the intervention; without a control group, it’s hard to rule out the possibility that participants taking creatine experienced improvements due to the passing of time, a “learning effect” from repeated testing. However, at least regarding the creatine stores, it seems likely that creatine supplementation was responsible for this. We can determine from this trial creatine was generally safe and feasible in AD patients, which was the study’s stated purpose. Furthermore, the magnitude of change (effect size) and variability (confidence intervals) provide data to inform sample sizes in future trials. Although we should stop short of using this study to say that creatine supplementation is directly responsible for the improvement in outcomes, these data are sufficient to generate a hypothesis that creatine may enhance creatine stores and cognition in AD patients.
Pathology of AD and Previous Creatine AD Research
Although causality claims are limited in a single-arm trial, AD pathology (14) provides a sound rationale for the use of creatine. In brief, there are two main proteins involved in AD: 1) amyloid beta protein fragments and 2) tau protein. Amyloid beta fragments are present in the brain, and although their function in healthy people is not well understood, they are thought to help direct neuronal movement, and their precursor (amyloid beta precursor protein) may aid in synaptic repair (15). Tau protein stabilizes and supports microtubules, which provide structure and support to neurons (16). In other words, amyloid beta fragments and tau proteins assist in the normal physiological function of neurons and information transmission. However, in AD, these proteins undergo modification, which disrupts brain function, such as ATP production (10). Specifically, amyloid beta fragments can clump together to form plaques between cells, affecting neuronal communication (17) and, in turn, memory and processing. Additionally, tau protein, like all proteins, has a specific amino acid sequence and then “folds” into a specific three-dimensional shape to carry out its function. However, in AD, an incorrect amino acid sequence can occur, causing the protein to misfold or become “tangled” which can disrupt neurons, impair their function, and accumulated tangles can lead to neuronal death (17). The exact cause of AD, other than advanced aging, identified lifestyle risk factors such as smoking, high blood pressure, diabetes, and obesity, and genetic predisposition, is not well understood (18). Furthermore, the interplay between amyloid beta and tau proteins is not fully understood, although amyloid beta plaque build-up may cause tau protein misfolding (17). The negative effects of amyloid beta plaque build-up and tau protein misfolding disrupt brain mitochondrial function, which is why generation of ATP and creatine stores are low and creatine may be effective. Prior to the current study, which has limited takeaways, creatine supplementation was shown to improve mitochondrial function and cognition in mice with AD (19).
Creatine, Cognition, and Neuroprotection in Humans
Although the reviewed study examined creatine in patients with AD, the hullabaloo surrounding creatine in recent years has focused on brain health in otherwise healthy adults. Currently, it is fair to say that the findings for creatine and cognition in healthy adults are equivocal, and if a benefit exists, it is likely small. A meta-analysis by Xu et al (4) found that creatine supplementation significantly improved memory (SMD = 0.31) but did not have significant effects on overall cognition, executive function, attention, or processing speed. Some sub-analyses in this meta-analysis were significant, as the authors noted “creatine supplementation significantly reduces processing speed time in female participants but does not have a significant effect in male participants.” However, the meta-analysis only included 16 studies, and this specific sub-analysis only included eight studies.
Overall, there is inconsistency in this body of literature, which to date, is too small to make definitive conclusions about creatine boosting cognition in healthy adults. For example, Moriarty et al (5 – MASS Review) carried out a 6-week double-blind placebo-controlled trial comparing 10 g/day of creatine monohydrate, 20 g/day of creatine monohydrate, or a placebo in women and men (19 – 33 years old, n = 30). The researchers found that neither creatine dosage improved any of the cognitive assessments (processing speed, episodic memory, or attention), nor did creatine improve oxygenation of the brain’s prefrontal cortex. However, it’s possible that creatine supplementation may have a positive effect on cognition in individuals who generally consume less creatine, such as vegetarians. In 2003, Rae et al (20) found, in a crossover design with a 5-week washout between phases, that individuals improved working memory more during six weeks of 5 g/d of creatine supplementation than with a placebo. However, this isolated finding has not been replicated. A more recent research (21) in a larger sample (n = 123) consisting of vegetarians and omnivores documented a positive effect of creatine using the same two cognitive tasks that Rae et al used. However, the effect was much smaller and was not influenced by diet (i.e., no further benefit to vegetarians). Despite vegetarians consuming less creatine on average, their brain creatine levels do not seem to significantly differ from omnivores (22). Therefore, while creatine may be beneficial for cognitive performance in conditions in which a brain creatine deficit is present, such as AD or Parkinson’s disease, I wouldn’t expect a huge boost in cognition for healthy vegetarians.
In a recent study by Korovljev et al (23), postmenopausal and perimenopausal women (n = 36) were divided into four groups receiving different creatine dosages, and changes in cognition and brain creatine levels were assessed before and after eight weeks of supplementation. The dosages were as follows: 1) 0.75g/d of creatine hydrochloride, 2) 1.5g/d of creatine hydrochloride, 3) 400 mg/d creatine hydrochloride + 400 mg/d creatine ethyl ester, or 4) placebo. All creatine groups showed a significant increase in brain creatine content, and there were no severe adverse events in these groups. Subjects in all creatine groups also experienced cognitive benefits to some degree, although not for every outcome. Specifically, the low-dose creatine hydrochloride (0.75g/d) led to improved cognition in some metrics of attention, processing speed, and reaction time; moderate dose of hydrochloride (1.5g/d) led to improved reaction time; and the hydrochloride + ethyl ester group experienced increased reaction time and alertness. This study suggests that creatine hydrochloride, at a very small dose, is beneficial for cognition. Creatine hydrochloride is purported to be more bioavailable than creatine monohydrate because of its increased solubility in water, but as noted in a review by Kreider et al (24), this notion dates back to a study in rats (25) that assessed tissue uptake of creatine hydrochloride but did not compare the uptake of creatine monohydrate. Furthermore, a recent study (26) in athletes demonstrated that 5 g/d of both forms led to comparable changes in performance and body composition. Given the lack of evidence of the benefits of creatine hydrochloride versus creatine monohydrate in the literature, we should look for replication of the present results before claiming the use of creatine hydrochloride for cognition. This is especially true given the low dosages used in this study. While creatine hydrochloride may be more soluble in water than monohydrate, the notion that you could get benefits at such a low dose of only 0.75g/d is a novel and surprising finding in healthy people.
Although the cognitive findings from Korovljev et al (23) look impressive on the surface, this study also reported an increase in brain creatine of ~9% in the 0.75g/d of hydrochloride group, ~7% in the 1.5g/d group, and ~11% in the hydrochloride + ethyl ester group. These findings seem to be inconsistent with the literature on creatine monohydrate supplementation at lower doses. Forbes et al reported (27) that studies with much higher dosages led to 3 to 10% increases in brain creatine. This includes Dechent et al (27), who reported an 8.7% average increase across all regions following 20 g/d of creatine monohydrate for four weeks. The increase in brain creatine reported by Korovljev et al is comparable to the results of the study by Smith et al (1) in AD patients, who often have lower brain creatine levels and received 20g/day. Overall, the Korovljev et al study reports a large boost in both cognition and brain creatine levels, but given the relatively low dose and alternative creatine form, we should wait for replication before using this study as the main justification for creatine and brain health. Additionally, with a sample size of 36 individuals and a huge number of outcomes, the probability of spurious findings in the study by Korovljev et al is quite high. The study design would have been strengthened considerably by only having two groups (one placebo and one with a substantial dose of creatine) to hone in on answering the question, “does creatine supplementation increase cognition?”
Next Steps
The obvious next step is to replicate the current study by Smith et al (1) but with a placebo group. That simple change will allow researchers to shed light on the question, “Does creatine supplementation increase creatine levels and enhance cognition compared to no supplementation in patients with AD?”
In healthy individuals, more trials similar to the one proposed for AD are needed. The current body of literature is heterogeneous, and I don’t see value in attempting to examine the “dose-response” of creatine, such as a 4-arm study comparing 20 g/d, 10 g/d, 5 g/d, and placebo, as that will split subjects between groups and decrease statistical power. More research is needed to determine whether creatine supplementation in healthy individuals enhances cognition. I would recommend studies comparing 10 g/d, a relatively high dose, since it may take more creatine to increase brain creatine content than muscle creatine content, versus a placebo for cognitive function over a longer term than most current literature (i.e., >16 weeks).
Application and Takeaways
Overall, the jury is still out on creatine for cognition, despite what the popular media reports. The benefits of creatine for cognition in healthy individuals are inconsistent and small (4). Given the hype, it may seem that I am being overly pessimistic, and I admit that it is generally in my nature to be skeptical, but I do not think the data is overly convincing…yet. Importantly, I believe that we are about to witness a huge boom in research in this area, and I have no idea whether my current opinion will hold in a few years.
Given that the present study is the first human trial on patients with AD, we should wait for a randomized controlled trial before making any confident claims. However, it is important to state that in young healthy individuals, older adults, and AD patients, creatine is generally safe without major adverse events, which means that creatine clears a huge hurdle for supplementation, especially when considering its potential use in clinical populations.
References
- Smith AN, Choi IY, Lee P, Sullivan DK, Burns JM, Swerdlow RH, Kelly E, Taylor MK. Creatine monohydrate pilot in Alzheimer’s: Feasibility, brain creatine, and cognition. Alzheimer’s & Dementia: Translational Research & Clinical Interventions. 2025 Apr;11(2):e70101.
- Burke R, Piñero A, Coleman M, Mohan A, Sapuppo M, Augustin F, Aragon AA, Candow DG, Forbes SC, Swinton P, Schoenfeld BJ. The effects of creatine supplementation combined with resistance training on regional measures of muscle hypertrophy: a systematic review with meta-analysis. Nutrients. 2023 Apr 28;15(9):2116.
- Gil A, Gonzalez DE, Hines K, Bonilla DA, Kreider RB. Safety of creatine supplementation: analysis of the frequency of reported side effects in clinical trials. Journal of the International Society of Sports Nutrition. 2025 Sep 30;22(sup1):2533688.
- Xu C, Bi S, Zhang W, Luo L. The effects of creatine supplementation on cognitive function in adults: a systematic review and meta-analysis. Frontiers in Nutrition. 2024 Jul 12;11:1424972.
- Moriarty T, Bourbeau K, Dorman K, Runyon L, Glaser N, Brandt J, Hoodjer M, Forbes SC, Candow DG. Dose–response of creatine supplementation on cognitive function in healthy young adults. Brain Sciences. 2023 Sep 1;13(9):1276.
- Giorgi C, Marchi S, Simoes IC, Ren Z, Morciano G, Perrone M, Patalas-Krawczyk P, Borchard S, Jędrak P, Pierzynowska K, Szymański J. Mitochondria and reactive oxygen species in aging and age-related diseases. International review of cell and molecular biology. 2018 Jan 1;340:209-344.
- Zorov DB, Juhaszova M, Sollott SJ. Mitochondrial reactive oxygen species (ROS) and ROS-induced ROS release. Physiological reviews. 2014 Jul;94(3):909-50.
- Ferrier CH, Alarcon G, Glover A, Koutroumanidis M, Morris RG, Simmons A, Elwes RD, Cox T, Binnie CD, Polkey CE. N-Acetylaspartate and creatine levels measured by 1H MRS relate to recognition memory. Neurology. 2000 Dec 26;55(12):1874-83.
- Prokopidis K, Giannos P, Triantafyllidis KK, Kechagias KS, Forbes SC, Candow DG. Effects of creatine supplementation on memory in healthy individuals: a systematic review and meta-analysis of randomized controlled trials. Nutrition reviews. 2023 Apr 1;81(4):416-27.
- Spuch C, Ortolano S, Navarro C. New insights in the amyloid‐beta interaction with mitochondria. Journal of aging research. 2012;2012(1):324968.
- Folstein MF, Robins LN, Helzer JE. The mini-mental state examination. Archives of general psychiatry. 1983 Jul 1;40(7):812.
- Weintraub S, Dikmen SS, Heaton RK, Tulsky DS, Zelazo PD, Bauer PJ, Carlozzi NE, Slotkin J, Blitz D, Wallner-Allen K, Fox NA. Cognition assessment using the NIH Toolbox. Neurology. 2013 Mar 12;80(11_supplement_3):S54-64.
- Taylor MK, Burns JM, Choi IY, Herda TJ, Lee P, Smith AN, Sullivan DK, Swerdlow RH, Wilkins HM. Protocol for a single-arm, pilot trial of creatine monohydrate supplementation in patients with Alzheimer’s disease. Pilot and Feasibility Studies. 2024 Feb 27;10(1):42.
- Zheng Q, Wang X. Alzheimer’s disease: insights into pathology, molecular mechanisms, and therapy. Protein & cell. 2025 Feb;16(2):83-120.
- Chen GF, Xu TH, Yan Y, Zhou YR, Jiang Y, Melcher K, Xu HE. Amyloid beta: structure, biology and structure-based therapeutic development. Acta pharmacologica sinica. 2017 Sep;38(9):1205-35.
- Barbier P, Zejneli O, Martinho M, Lasorsa A, Belle V, Smet-Nocca C, Tsvetkov PO, Devred F, Landrieu I. Role of tau as a microtubule-associated protein: structural and functional aspects. Frontiers in aging neuroscience. 2019 Aug 7;11:204.
- Bloom GS. Amyloid-β and tau: the trigger and bullet in Alzheimer disease pathogenesis. JAMA neurology. 2014 Apr 1;71(4):505-8.
- Silva MV, Loures CD, Alves LC, De Souza LC, Borges KB, Carvalho MD. Alzheimer’s disease: risk factors and potentially protective measures. Journal of biomedical science. 2019 May 9;26(1):33.
- Snow WM, Cadonic C, Cortes-Perez C, Chowdhury SK, Djordjevic J, Thomson E, Bernstein MJ, Suh M, Fernyhough P, Albensi BC. Chronic dietary creatine enhances hippocampal-dependent spatial memory, bioenergetics, and levels of plasticity-related proteins associated with NF-κB. Learning & Memory. 2018 Feb 1;25(2):54-66.
- Rae C, Digney AL, McEwan SR, Bates TC. Oral creatine monohydrate supplementation improves brain performance: a double–blind, placebo–controlled, cross–over trial. Proceedings of the Royal Society of London. Series B: Biological Sciences. 2003 Oct 22;270(1529):2147-50.
- Sandkühler JF, Kersting X, Faust A, Königs EK, Altman G, Ettinger U, Lux S, Philipsen A, Müller H, Brauner J. The effects of creatine supplementation on cognitive performance—a randomised controlled study. BMC medicine. 2023 Nov 15;21(1):440.
- Solis MY, de Salles Painelli V, Artioli GG, Roschel H, Otaduy MC, Gualano B. Brain creatine depletion in vegetarians? A cross-sectional 1H-magnetic resonance spectroscopy (1H-MRS) study. British journal of nutrition. 2014 Apr;111(7):1272-4.
- Korovljev D, Ostojic J, Panic J, Ranisavljev M, Todorovic N, Nedeljkovic D, Kuzmanovic J, Vranes M, Stajer V, Ostojic SM. The Effects of 8-Week Creatine Hydrochloride and Creatine Ethyl Ester Supplementation on Cognition, Clinical Outcomes, and Brain Creatine Levels in Perimenopausal and Menopausal Women (CONCRET-MENOPA): A Randomized Controlled Trial. Journal of the American Nutrition Association. 2025 Aug 21:1-2.
- Kreider RB, Jäger R, Purpura M. Bioavailability, efficacy, safety, and regulatory status of creatine and related compounds: a critical review. Nutrients. 2022 Feb 28;14(5):1035.
- Alraddadi EA, Lillico R, Vennerstrom JL, Lakowski TM, Miller DW. Absolute oral bioavailability of creatine monohydrate in rats: debunking a myth. Pharmaceutics. 2018 Mar 8;10(1):31.
- Londoño-Velásquez D, Zuluaga-Narváez Y, Rojas-Posada L, Kammerer-López M, Cardona-Arenas ÓM, Quiroz-Bastidas OL, Quintero-Velásquez MA, Rojas-Jaramillo A, Kreider RB, Bonilla DA. Creatine monohydrate versus creatine hydrochloride on strength and body composition in elite team-sport athletes: A placebo-controlled randomized clinical trial comparing low dosages. Journal of the International Society of Sports Nutrition. 2025 Sep 30;22(sup1):2533658.
- Forbes SC, Cordingley DM, Cornish SM, Gualano B, Roschel H, Ostojic SM, Rawson ES, Roy BD, Prokopidis K, Giannos P, Candow DG. Effects of creatine supplementation on brain function and health. Nutrients. 2022 Feb 22;14(5):921.
- Dechent P, Pouwels PJ, Wilken B, Hanefeld F, Frahm J. Increase of total creatine in human brain after oral supplementation of creatine-monohydrate. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology. 1999 Sep 1;277(3):R698-704.
Leave a Reply